Government Oversight effort is gaining momentum as Congress introduces legislation to provide increased Federal oversight of prescription opioid treatment and assistance to States in reducing opioid abuse, diversion, and deaths.
On February 13, 2013 the 113th Congress, First Session, introduced H.R. 672: Prescription Drug Abuse Prevention and Treatment Act of 2013. The basis for this Bill rests upon the following Congressional findings:
(1) Nonmedical use of prescription pain relievers is a matter of increasing public health concern. According to the Substance Abuse and Mental Health Services Administration, the proportion of all substance abuse treatment admissions aged 12 or older that reported any pain reliever abuse increased more than 400 percent between 1998 and 2008, from 2.2 to 9.8 percent.
(2) In 2008, among the population of the United States aged 12 or older, nonmedical use of prescription pain relievers was the second most prevalent type of illicit drug use, after marijuana use.
(3) When used properly under medical supervision, prescription opiates enable individuals with chronic pain to lead productive lives. However, when taken without a physician’s oversight and direction, opiates can cause serious adverse health effects, resulting in dependence, abuse, and death.
(4) As with any controlled substance, there is a risk of abuse of methadone and other opiates.
(5) Methadone is an extensively tested, federally approved, and widely accepted method of treating addiction to prescription pain relievers or opiates.
(6) For more than 30 years, this synthetic prescription drug has been used for pain management and treatment for addiction to heroin, morphine, and other opioid drugs.
(7) The efficacy and lower cost of methadone has resulted in its being prescribed for pain management.
(8) Prescriptions for methadone have increased by nearly 700 percent from 1998 through 2006.
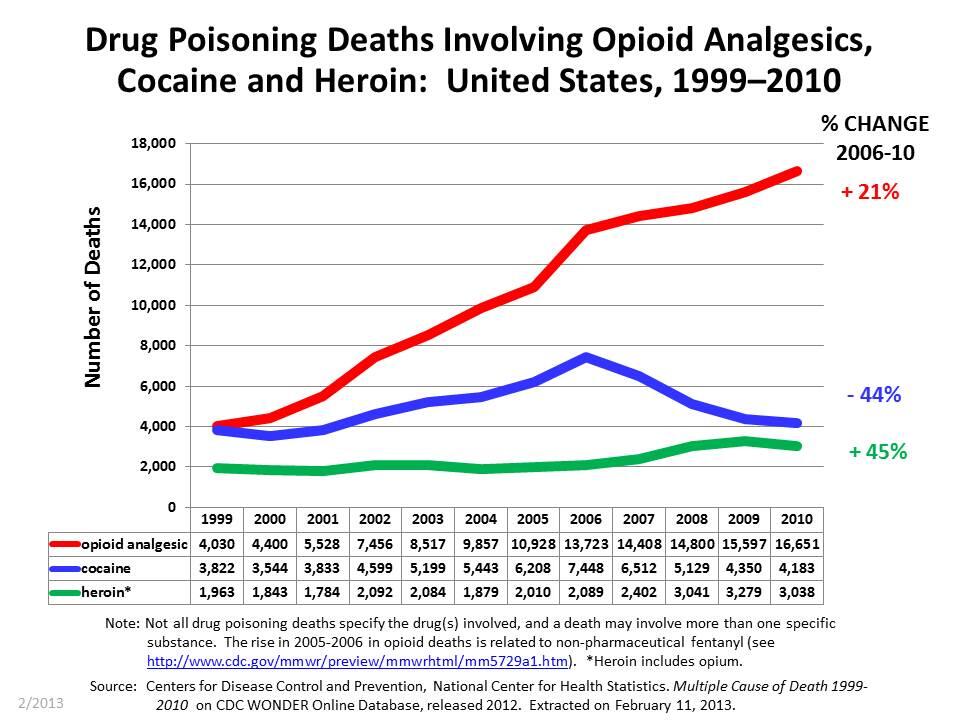
(9) According to the Centers for Disease Control and Prevention, the number of poisoning deaths involving methadone increased nearly 7-fold from almost 790 in 1999 to almost 5,420 in 2006, which is the most rapid increase among opioid analgesics and other narcotics involved in poisoning deaths.
(10) The age-specific rates of methadone death are higher for persons age 35 to 44 and 45 to 54 than for other age groups. However, the rate of methadone deaths in younger individuals (age 15 to 24) increased 11-fold from 1999 through 2005.
(11) Deaths from methadone and other opiates may actually be underreported. There is no comprehensive database of drug-related deaths in the United States.
(12) The lack of standardized reporting by Medical Examiners precludes a uniform definition of ‘cause of death’ on death certificates.
(13) The Controlled Substances Act (21 U.S.C. 801 et seq.) requires that every person who dispenses or who proposes to dispense controlled narcotics, including methadone, whether for pain management or opioid treatment obtain a registration from Drug Enforcement Administration. Unfortunately there is no requirement as a condition of receiving the registration that these practitioners receive any education on the use of these controlled narcotics, including methadone.
(14) Current Federal oversight of methadone and other opioids is inadequate to address the growing number of opioid-related overdoses and deaths.
(15) Federal legislation is needed to avert opioid abuse, misuse, and death, without reducing patient access to needed care.
Please click on the following link to review the complete H.R. 672: Prescription Drug Abuse Prevention and Treatment Act of 2013: H.R 672.
Legislation is at the forefront of controversy as many view this type of action as nothing more than big government interfering with basic patient care rights along with the roles and responsibilities of the Doctor. The following link discusses some of these issues: Tightening the Lid on Pain Prescriptions.
On January 25, 2013 an advisory panel to the FDA recommends additional restrictions on opioids as reviewed in this link: FDA Panel Recommendations.
To better understand this growing concern I’ve put together the following list of those familiar terms we have heard connected to painkillers, but unsure what they really mean:
Abuse: Self-administration of medications to alter one’s state of consciousness (“get high”). This is an intentional, maladaptive pattern of use of a medication (whether legitimately prescribed or not) leading to significant impairment or distress—such as repeated failure to fulfill role obligations, recurrent use in situations in which it is physically hazardous, multiple legal problems, and recurrent social and interpersonal problems—occurring over a 12-month period.
Addiction: A primary, chronic, neurobiological disease, with genetic, psychologic, and environmental factors influencing its development and manifestations. Addiction is characterized by the 4 C’s—behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.
Chemical coping: Reliance on a drug for psychological stability.
Diversion: Redirection of a prescription drug from its lawful purpose to illicit use; can be done with criminal intent.
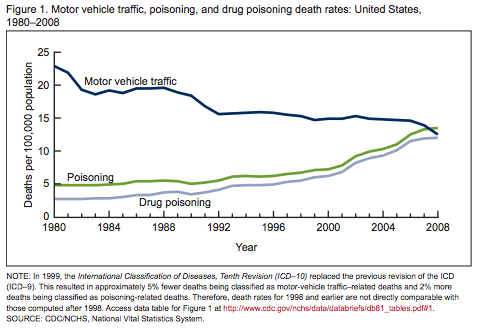
Drug poisoning: Exposure to a natural or manmade substance that has an undesirable effect, often fatal; includes drug overdoses resulting from misuse or abuse. In the U.S., drug overdose deaths were second only to motor vehicle crash deaths among leading causes of unintentional injury death in 2007.
Misuse (noncompliant use): The intentional or unintentional use of a prescribed medication in a manner that is contrary to directions, regardless of whether a harmful outcome occurs. Misuse can be grouped into several categories:
- Not taking the medication according to the prescription
- Unsanctioned use (running out early; bingeing)
- Altering the route of delivery (injecting, crushing tablets, snorting, chewing)
- Accessing drugs from other sources (friend, the street, other doctors)
- Drug-seeking behavior (anger, harassing office staff for fit-in appointments)
- Reluctance to use other methods of pain management
Non-medical use (prescription drug abuse, illicit use): Intentional or unintentional use of legitimately prescribed medication in an unprescribed manner for its psychic effect (either experimentation or recreationally), deciding to increase the dose of one’s own medication, unknowingly taking a larger dose than directed, engaging in a suicidal attempt or gesture, and inadvertent poisoning. The non-medical use of prescription medications implies that the person is using the drug for reasons other than those indicated in the prescribing literature or other off-label uses prescribed by a clinician. Nonmedical use includes procurement of drugs for abuse, bartering, suicide, homicide, or accidental ingestion.
Pharming: Coined by teenagers, “pharming” is the term used to describe raiding the medicine closet for prescription medicines, popularly known as “pilz.” At “pharm” parties, various prescription drugs are tossed together in a big bowl of “trail mix” and consumed by the handful.
Physical dependence: A state of adaptation manifested by a drug class-specific withdrawal syndrome that occurs by abrupt cessation of a drug, rapid dose reduction, decreasing levels of the drug in the blood, and/or administration of an antagonist resulting in dysphoric signs and symptoms generally the opposite of the desired drug effect, and tolerance defined by adaptation so that that increasing doses of a drug is needed to achieve the same desired effect. Physical dependence involves the related phenomenon of withdrawal and tolerance.
Prescription medications: Pharmaceuticals dispensed by a pharmacist on the presentation of a prescription written by a physician, dentist, or other health care provider who is legally authorized to write prescriptions.
Pseudoaddiction: Occurs when patients with inadequately treated pain exhibit drug-seeking behavior similar to that of addiction. This behavior resolves with reasonable dose increases as opposed to “out of control” or “compulsive” use reflecting addictive drug-seeking behavior which remains the same or worsens.
Self-medication: Use of a drug without consulting a health care professional to alleviate stressors or disorders such as depression and anxiety.
Substance Use Disorder (SUD): A condition involving the intoxication, withdrawal, abuse or dependence upon, a substance with defined abuse or dependence potential, including alcohol, meeting the criteria for clinical diagnosis delineated by the current Diagnostic and Statistical Manual (DSM) and/or the current International Classification of Diseases (ICD).
Tolerance: A state of adaptation in which exposure to a given dose of a drug induces changes that result in diminution of one or more of the drug’s effects over time.
Withdrawal: A variety of unpleasant symptoms (e.g., difficulty concentrating, irritability, anxiety, anger, depressed mood, sleep disturbance, and craving) that occur after use of an addictive drug is reduced or stopped. Withdrawal symptoms are thought to increase the risk for relapse.
The following link is an excellent source for more information: American College of Preventive Medicine.
With all of the “baggage” associated with opioids we now have something called “Opioidphoboia”. Long term opioid therapy can provoke anxiety in patients and providers alike. Patients may not be comfortable with opioid pain management because they see opioid use as a personality flaw due to the societal stigma these medications have. Click on Access to pain management hampered by addiction fears, government relations to learn more.
Further complication resides in the fact that each State has several types of laws dealing with the practice of opioids. The following link contains all such laws for each State: Centers for Disease Control and Prevention.
In the State of California, a bill known as AB Assembly 889 recently passed out of Assembly Appropriations Committee. This legislation was amended in the State of California on May 2, 2013. This important legislation will give people suffering from chronic pain quicker access to needed pain medication as prescribed by their healthcare provider without the usual obstacles and delays from insurance carriers. The following link will provide particulars of this legislation: California’s AB 889.
Government Oversight is another complicated strand with the painweb. Among the core problems for why Congress has become directly involved can be seen in the following chart illustrating the recent explosive sales of opioids:
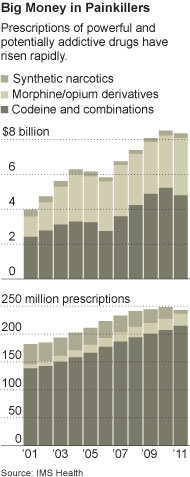
Click on The New York Times to read more.
This significant increase in sales of opioids when combined with the alarming morality rates from opioid overdose further complicates the painweb.
The mortality rate from opioid overdose is another core problem. According to the Centers for Disease Control and Prevention (CDC), deaths from unintentional drug overdoses in the United States have been rising steeply since the early 1990s and are the second-leading cause of accidental death, with 27,658 such deaths recorded in 2007. That increase has been propelled by a rising number of overdoses of opioids (synthetic versions of opium), which caused 11,499 of the deaths in 2007 — more than heroin and cocaine combined. Visits to emergency departments for opioid abuse more than doubled between 2004 and 2008, and admissions to substance-abuse treatment programs increased by 400% between 1998 and 2008, with prescription painkillers being the second most prevalent type of abused drug after marijuana. The following link will provide more details: New England Journal of Medicine; A Flood of Opioids, a rising Tide of Deaths.
Interestingly, pain research accounts for only about 1% of research grants awarded by the National Institutes of Health (NIH) while the 2012 annual cost of chronic pain is as high as $635 Billion a year which exceeds yearly costs for cancer, heart disease and diabetes combined. The following link reviews the details: Federal Spending to Treat Chronic Pain.
The American Academy of Pain Medicine reports that the most common type of chronic pain is low back pain. This group represents 27% of the 100 million Americans suffering from chronic pain. Second place is tied with chronic pain from severe headaches, or migraines 15% and neck pain 15%. It’s no surprise that chronic low back pain and chronic neck pain may have a direct physiological correlation. These top two chronic pain categories (low back pain and neck pain) represent 42% of all chronic pain sufferers. The following link provides more specifics: AAPM.
Despite the significant size of chronic low back pain and neck pain sufferers, the National Institutes of Health (NIH) does not spend a single penny for research in this particular category. Keep in mind that the NIH spends $30.9 billion annually for medical research with just 1% allocated for all chronic pain. The top 2 causes of chronic pain (low back pain and neck pain) don’t get one cent. The following link lists all the NIH medical research spending by category: NIH Categorical Spending.
Warranties for implanted medical devices?? Read the following: Implanted medical device warranties.
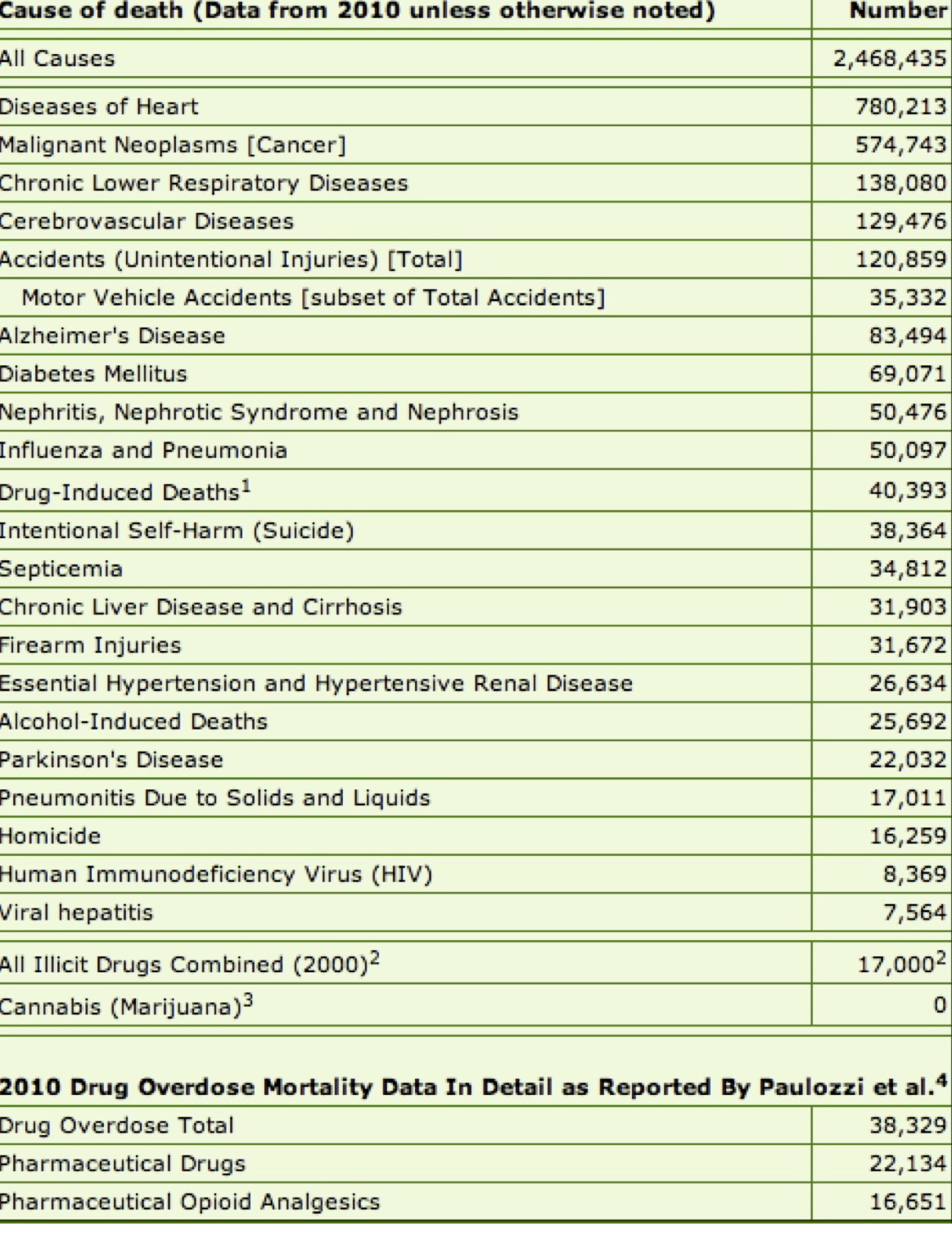
Here’s another fact representing the the devastating number of deaths from drugs as compared to other causes of deaths:
What about America’s “War on Drugs”?
After 40 years and costing over $1.5 Trillion, it’s been a costly, losing “War”. The following is a 40-year “War on Drugs” Presidential perspective brief:
1971 “War on Drugs” officially begins under President Nixon:
In June 1971, President Nixon declared a “war on drugs.” He dramatically increased the size and presence of federal drug control agencies, and pushed through measures such as mandatory sentencing and no-knock warrants. Nixon temporarily placed marijuana in Schedule One, the most restrictive category of drugs, pending review by a commission he appointed led by Republican Pennsylvania Governor Raymond Shafer. In 1972, the commission unanimously recommended decriminalizing the possession and distribution of marijuana for personal use. Nixon ignored the report and rejected its recommendations. His first-year “War on Drugs” budget was $100 Million.
Each subsequent Presidential Administration “shifted” the “War on Drugs”:
In January 1977, President Jimmy Carter was inaugurated on a campaign platform that included marijuana decriminalization.
President Reagan in 1981 expands incarcerations by adopting a zero-tolerance, “Just Say No” campaign. “War on Drugs” success measurement was those incarcerated.
President George H.W. Bush during his 1989 “Crack speech” pledged one billion dollars to escalate he drug war because “we need more jails, more prisons, more courts and more prosecutors.” President H.W. Bush re-defined the irrational zero tolerance drug policies of the times that put ideology and politics above science and health
Efforts to eradicate opium at its source remains unsuccessful:
The 1994 President Clinton Administration orders a shift in policy away from the anti- drug campaigns of previous administrations. Instead the focus includes “institution building” with the hope that by “strengthening democratic governments abroad, [it] will foster law-abiding behavior and promote legitimate economic opportunity.”
President George W. Bush arrived in the White House as the drug war was running out of steam – yet he allocated more money than ever to it in 2009. His drug czar, John Walters, zealously focused on marijuana and launched a major campaign to promote student drug testing. While rates of illicit drug use remained constant, overdose fatalities rose rapidly. The era of George W. Bush also witnessed the rapid escalation of the militarization of domestic drug law enforcement. By the end of Bush’s term, there were about 40,000 paramilitary-style SWAT raids on Americans every year – mostly for nonviolent drug law offenses, often misdemeanors.
Politicians now (2014) routinely admit to having used marijuana, and even cocaine, when they were younger. President Barack Obama candidly discussed his prior cocaine and marijuana use: “When I was a kid, I inhaled frequently – that was the point.”
The assault on American citizens, however, has persisted through 2014. Despite advocating for reforms – such as reducing the crack/powder sentencing disparity, ending the ban on federal funding for syringe access programs, and supporting state medical marijuana laws – President Obama has yet to shift drug control funding to a health-based approach.
The “War on Drugs” continues to this day. By comparison, the U.S. spent $15.6 Billion in just one year, 2011, for the “War on Drugs.
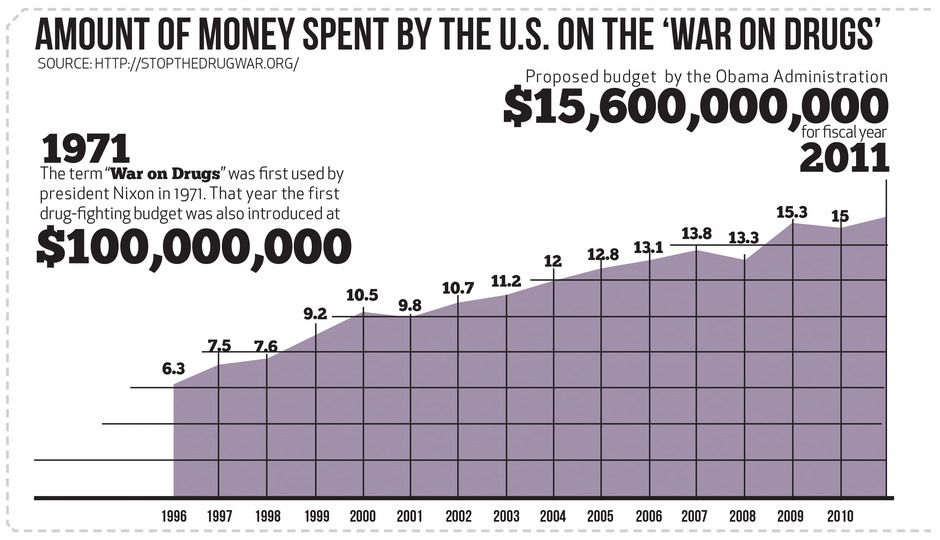
From 1970 through 2010 the “War on Drugs” has cost America $1.5 Trillion.
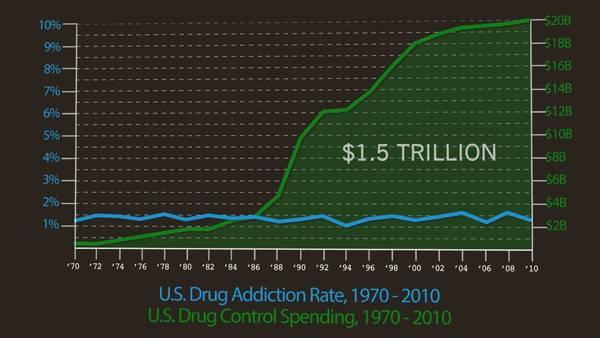
Despite the mega-trillion dollar spending, America’s addiction rate remains unchanged while the deaths as a result of prescription and illicit drugs remain at record levels.
The FDA approves ZOHYDRO……the new SUPER Opioid Painkiller.
* 10 x the power of other painkillers like Vicodin.
* A child could die from ingesting just one capsule &
an adult new to opioids could die from just
2 capsules.
* Nearly 60 percent of all drug overdoses are from FDA-
approved prescription medications. Zohydro will likely
trigger a spike in deaths caused by opioids. Keep in mind
in 1999 about 4,000 people died from opioid poisoning
with 17,000 deaths in 2010!!
* Over 40 Industry experts along with Congressional
Representatives & State Attorney Generals urged the
FDA to say NO to Zohydro.
* The FDA chose NOT to listen to its own advisory panel,
which voted 11-2 AGAINST approving Zohydro.
* Why did the FDA approve Zohydro? Zogenix, the drug
company maker, argued its safer than the existing opioid
alternatives because it doesn’t contain acetaminophen.
Zohydro is expected to be available next month.
Read the complete Zohydro story at the following link: Zohydro

Why are opioids potentially unsafe??
Here are a few of the well-known reasons:
- may slow down the part of the brain that controls breathing which can result in death
- may slow down the part of the brain that controls breathing which can result in death
- may develop addiction and/or tolerance, leading to increased use of more opioids which can lead to overdose
- abusing them can permanently damage veins and organs.
- can cause psychological depression / mood disorders
Here is the NOT well-known reason:
Prior to obtaining FDA approval, research is done on all medications to produce evidence of the long-term effectiveness and safety of medications. Particular scrutiny is given to medications used for managing long-term chronic conditions.
Person-time is the research measurement used to estimate the actual time in years, months, or days that all persons contributed to the study-observation of a particular medication. Analysis of the person-time results is used to determine the safety & effectiveness of the trialled medication.
Check out these examples:
Hypertensive medications…………..1,800,000 person-years were studied
Cholesterol medications……………..750,000 person-years were studied
NSAIDS (aspirin & ibuprofen)……100,000 person-years were studied
Opioids ………………………………………1,500 person-years were studied
Opioids by comparison, have only a meager person-years observation. The studies of chronic opioid therapy are too short to evaluate long-term effectiveness, and too small to adequately evaluate safety. Source: Opioids for Chronic Pain
Opioids, though FDA approved, are one of the most potentially dangerous medications prescribed today has actually been studied the least. What do you think?
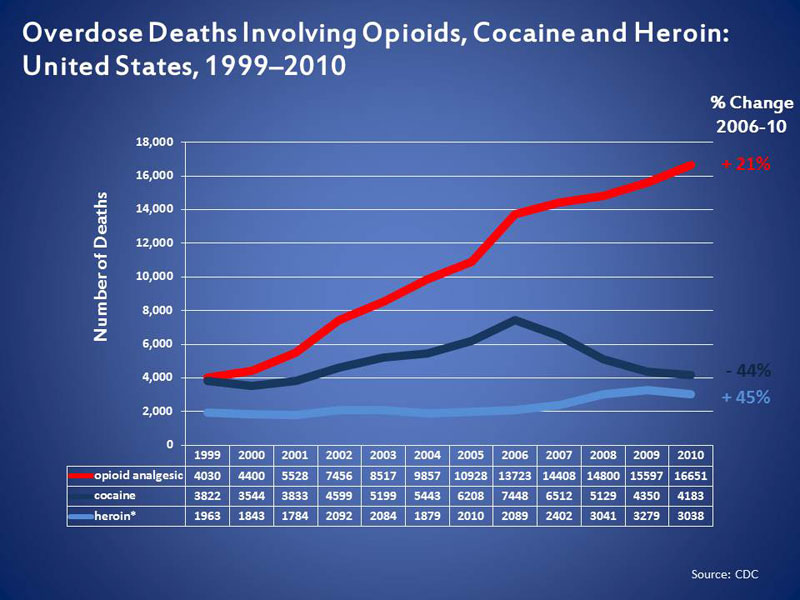
White House report on Opioid Overdoses:
More Americans are using and dying from prescription painkillers than from heroin. According to the Centers for Disease Control and Prevention (CDC), we’ve seen roughly a 20 percent increase in overdose deaths involving prescription painkillers since 2006. In 2010, there were over 16,000 drug poisoning deaths involving prescription painkillers. There were about 3,000 drug poisoning deaths involving heroin that same year.
{kind=link}
Click the link below to read this full White House report:
The White House Report About Opioid Overdoses
Ohio House passes bill to make prescription painkiller abuse part of schools’ health curricula.
Under the proposal passed by the House on Wednesday, March 12, 2014, schools within the State of Ohio would be required to update their health curricula with information about the addictive properties of prescription opioids and their links to heroin.
Click the link below to learn more:
Ohio’s prescription painkiller abuse health curricula
Zohydro Manufactured by Same Company That Makes Addiction Medicine
OUTRAGEOUS!!
Zohydro is made by the same company, Zogenix, that manufactures Vivitrol, a drug used to TREAT patients ADDICTED to opioids as reported by The New York Times.
So, we’re ready to unleash this dangerously powerful painkiller while we’re trending more deaths each year from prescription drug overdose than automobile traffic accidents!

Click the following to read more: Overdose rates
What is Zohydro?
It’s a super-opioid painkiller that has been FDA approved, shipped and ready for sale. Zohydro is 10 x the power of other painkillers like Vicodin. A child could die from ingesting just one capsule & an adult new to opioids could die from just 2 capsules. Check out Zohydro’s Warning Label below:


Why was Zohydro approved?
The Food and Drug Administration (FDA) claims that daily, around-the-clock, long-term treatment cannot be treated with our arsenal of existing available painkillers.

Click the following link to read more: Zohydro
Safety Claims:
Zogenix, Zohydro’s manufacturer, is publicizing its efforts to make sure the drug is used safely. The company’s approach involves the use of “safety monitoring boards”. Exactly who will be monitored (patients, doctors, or pharmacies) and how will they monitor (reviewing confidential doctor-patient medical files, dispensed prescriptions, sales data, direct contact) has not been disclosed. Experts say there is little evidence that the so-called “safe board” will ensure Zohydro is used appropriately. Critics point out the fact that 5 out of 7 experts on the “safe board” have previously received consulting payments from the company. All “safe board” panel members will be compensated for quarterly meetings to review Zohydro data. In essence, the claim has been made stating this external “safe board” panel of independent people is not independent, but are working directly for Zogenix. Furthermore, critics raise concern about the “safe board’s” level of authority or power whatsoever.
Click the following link to read more: Zohydro Safe Board
Zogenix’s multiple roles in the world of painkillers is troubling to say the least.
One thing that is certain……the revenues & profits to be generated from the new super-opioid painkiller Zohydro along with their opioid addiction drug, Vivitrol, will insure a HEALTHY balance sheet and ROI for Zogenix.
Unprecedented Action!!
The State of Massachusetts bans the sales of FDA approved super-opioid Zohydro. Click the following link to read more: No Zohydro

The Zohydro fight intensifies and get’s ugly as the argument takes on a politicizing slant. Once again, creating distraction from the logical decision adds complication & delay. Click on the following link to read the full story: Heroin in a Capsule?
FDA rejects new combination narcotic painkiller: Moxduo
Read the following link to gain insight on the FDA’s likely future direction concerning opioids: Long-Term Opioid Use Questioned for Chronic Pain
Opioid pain medication may soon be regulated
“Why should I care about the Opioid epidemic problem?” “The Opioid epidemic problem affects a select-few-celebrity-types and drug addicts.” “I’m neither, so it’s not my problem” you say…..well, think again.
If you or a family member visit your dentist regularly, or seek medical treatment from your primary care physician for a painful knee injury, sprained ankle, etc., then YOU MUST CARE.
What’s the Opioid epidemic about?
*Deaths:
Each day, 46 people die from an overdose of prescription painkillers in the US with another 54 people dying everyday from illegal drug overdosing. Overdosing is now the leading cause of accidental death in the United States, accounting for more deaths than traffic fatalities or gun homicides and suicides. Fatal overdoses from opiate medications such as oxycodone, hydrocodone, and methadone have quadrupled since 1999, accounting for an estimated 16,651 deaths in 2010.
Click on the following links to read more:
100 Americans die of drug overdoses each day
*Increasing availability of opioids:
In 2011, about 131 million prescriptions for hydrocodone-containing pain medications were written for about 47 million patients, according to government estimates. That amounts to about 5,000,000,000 (billion) pills; just one opioid pain medication in just one year!
Click on the following link to read more:
FDA urging tighter rein on painkillers
Between 1991 and 2010, prescriptions for opioid analgesics increased from about 75.5 million to 209.5 million.
Click on the following link to read more:
*Where you live in the US influences opioid availability:
U.S. health care providers wrote 259 million prescriptions for opioid painkillers in 2012, enough to give a bottle of the pills to every adult in the country. But your chances of ending up with those pills – and the risks that come with them – depend a lot on where you live, says a new report from the federal Centers for Disease Control and Prevention.
Click on the following link to read more:
*Cost:
It is estimated that substance abuse costs the United States in excess of $600 billion annually in health, crime and lost productivity costs — and this is nothing compared to the toll it takes on the families, friends, schools and communities affected.
Click on the following link to read more:
What’s the connection between your Dentist & Primary Care Physician and the Opioid epidemic problem??
Most prescription painkillers are prescribed by primary care and internal medicine doctors and dentists, not specialists. Roughly 20% of prescribers prescribe 80% of all prescription painkillers.
The records show that approximately 56 percent of painkiller prescriptions were given to patients who had filled another prescription for pain from the same or different providers within the past month.
In addition, nearly 12 percent of opioids prescribed were to young people aged 10-29. Most of these were hydrocodone and oxycodone-containing products, like Vicodin and Oxycontin. Dentists were the main prescribers for youth aged 10-19 years old. Nearly 46 percent of opioid prescriptions were given to patients between ages 40 and 59, and most of those were from primary care providers.
Click on the following links to learn more:
Analysis of Opioid prescription practices raise concerns
Opioids prescribing by dentists
Prevention of prescription opioid abuse: the role of the Dentist
What should I know about Opioids?
DON’T TAKE OPIOIDS IF:
-YOU’RE TAKING BENZODIAZEPINES: a class of drugs primarily used for treating anxiety (xanax, valium, & klonopin to name a few).
-YOU DRINK ALCOHOL
-You have been diagnosed with CLINICAL DEPRESSION!
It has been proven that the synergistic effect of combining opioids with benzodiazepines, alcohol, or anti-depression medication significantly increases the chance of accidental overdose resulting in death.
Research supports that drugs often prescribed for mental health conditions were involved in a significant number of pharmaceutical overdose deaths. Benzodiazepines (anti-anxiety drugs) were involved in nearly 30 percent (6,497) of these deaths; antidepressants in 18 percent (3,889), and antipsychotic drugs in 6 percent (1,351).
Click on the link below to learn more:
Opioids drive continued increase in drug overdose deaths
Don’t be fooled into thinking opioids are safe because a doctor prescribes them!!
Click on the link below to learn more:
Why doctors prescribe opioids to patients they know they are abusing them
So what’s being done about the Opioid epidemic??
Experts within the professional medical community disagree as to what to do about the opioid epidemic. Two opposing prestigious professional medical groups have begun a bitter battle.
Click on the following links to read their position:
PROP (Physicians for Responsible Opioid Prescribing) Position:
AMA (American Medical Association) Anti PROP Position:
What these two groups do agree on is that there’s insufficient study / data / research regarding long term opioid therapy.
Click on the following link to read more:
New Rules for Hydrocodone
After 10 years of formal debate and 15 years since the idea was first proposed, the strong opioid hydrocodone combination painkillers are finally being reclassified from the more-permissive Schedule III to the more-restrictive Schedule II category.
The change, effective October 6, 2014, won’t solve all the overuse/misuse problems associated with this potentially addictive opioid narcotic. This important step will help reduce the tragic accidental overdose death rate from opioid painkillers which now claims over 16,000 Americans annually.
Hydrocodone was already rightfully categorized as Schedule II. Oddly, in 1971 hydrocodone (at lower strength) when combined with another pain-killing drug, such as acetaminophen, was allowed to be placed in the less-restrictive Schedule III. In retrospect, it appears that this particular controlled substance legislation proved to be absolutely wrong as it contributed to our current national opioid overdose epidemic.
Click on the following link to read more:
D.E.A. to Allow Return of Unused Pills to Pharmacies
Concerned by rising rates of prescription drug abuse, the Drug Enforcement Administration announced Monday that it would permit consumers to return unused prescription medications like opioid painkillers to pharmacies.
The move is intended to help reduce stockpiles of unneeded medicines in homes, which are often pilfered by teenagers. Under the new regulation, patients and their relatives will also be allowed to mail unused prescription drugs to an authorized collector using packages to be made available at pharmacies and other locations, like libraries and senior centers.
The new regulation, which will go into effect in a month, covers drugs designated as controlled substances. Those include opioid painkillers like OxyContin, stimulants like Adderall and depressants like Ativan.
Until now, these drugs could not legally be returned to pharmacies. The Controlled Substances Act allowed patients only to dispose of the drugs themselves or to surrender them to law enforcement.
While many questions remain as to how this government program will be managed and enforced, the effort to reduced “unused” prescriptions medications makes sense. Perhaps they should add a “refund” component to the program? As an incentive to return potential dangerous prescription medications, like opioids, give a “cash refund” on unused pill quantities turned in.
Click on the following link to learn more:
D.E.A. to Allow Return of Unused Pills to Pharmacies

Change at the top requested at the FDA

Anti-addiction groups call for the FDA Commissioner to step down.
Finally, a key step in the right direction.
Click on the following link to read more:
Call for the FDA Commissioner to step down
2016 Presidential Cycle
The Opioid Prescription Drug, Chronic Pain, Disability worsening crisis will be a National Healthcare topic the presidential candidates, pundits and media will frequently visit during the campaign cycle.
The INCREDULOUS & MALICIOUS comments made by Senator Rand Paul during a recent breakfast in New Hampshire concerning those living with disabilities has set the tone for an antagonistic debate.
Here is what Senator Rand Paul said:
“You know, the thing is is that with all of these programs,
there’s always somebody who’s deserving and everybody in this room knows somebody who is gaming the system,” said Paul. “What I tell people is, ‘If you look like me and you hop out of your truck, you shouldn’t be getting a disability check.’ You know, over half the people on disability are either anxious or their back hurts. Join the club! [the group laughs] Who doesn’t get up a little anxious for work every day and their back hurts?! Everybody over 40 has a back pain.”
-Rand Paul, Senator
Click on the following link to hear Senator Paul’s speech:
Senator Rand Paul’s Disability Speech
Rand Paul as a Senator and Physician should be uniquely qualified to understand and help solve problems associated with Disability and Chronic Pain. How disappointing that Senator Paul chose such an untruthful & hurtful tact.
Senator Paul…..an apology is expected for fueling these misconceptions.
Why “The War on Drugs” is NOT a war…..

Opioid Painkiller Heroin Epidemic
Those who continue to gain the most are the same entities that created the problem. It just so happens these are the same key positions that have the authority to fix what’s broken….

CDC Draft Opioid Guidelines Ignite Controversy

American Medical Association votes to BAN prescription drug commercials

Nation’s Top Drug Official Calls War on Drugs a Failure


PATIENTS PRESCRIBED OPIOIDS for the first time would be limited to a seven-day supply and any individual admitted to the emergency room with an apparent drug overdose would be required to undergo a substance abuse evaluation within 24 hours, under a redrafted House bill.

Moments after posting the Opioid Abuse Bill (above)…..the following article is published explaining Painkiller politics:
Painkiller politics: Efforts to curb prescribing under fire

Painkiller Politics makes one point crystal clear: agreement exists among politicians, Big Pharma and special interest groups to not solve our Chronic Pain-Opioid Addiction epidemic.
CDC announces & implements new Opioid Prescribing Guidelines
Click on the following CDC link to read specifics about the new guidelines:
CDC Opioid Prescribing Guidelines


As this controversial topic continues to worsen amidst growing complication, there are some excellent additional internet resources:
The Prevention Coalition is one such resource. The Prevention Coalition was founded by a group of retired school counselors and therapists to provide an accessible drug use and abuse prevention resource for parents, teachers, counselors and other concerned adults.

Click on the following link to visit The Prevention Coalition:
Medical Marijuana is dominating the political-legal landscape

33 States have legalized Medical Marijuana (As of April 2019)…..
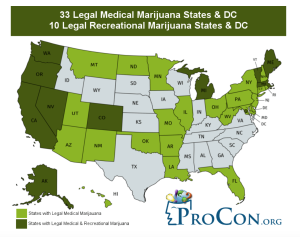
As more States legalize Medical Marijuana, the Federal Government will need to address existing Federal laws banning marijuana (including Medical Marijuana) while over 2/3 of the Nation has legalized Medical Marijuana at the State level.
Click on the following link to hear a compelling Medical Marijuana interview with an Ex-SC Senator’s wife:
Medical Marijuana riveting testimony
mypainweb continues to update you on these controversial topics.
If you, or a loved one, should face the reality of being prescribed opioids for pain, then you must take on the added responsibility to understand opioids.
Many tragic opioid outcomes start with a simple, innocent looking opioid prescription from your doctor handed to you.
Opioids are not a magic pill. They work by changing the person. Opioids are powerful and must be understood and respected.
Want to know more about opioids? Visit mypainweb.
mypainweb will continue to monitor Government Oversight as it relates to chronic pain and post updates as they unfold.